
The Ebola outbreak that is tearing through the Democratic Republic of the Congo (DRC) is already the third largest on record. Scientists are scrambling to model the size of the outbreak—caused by the rare Bundibugyo virus—based on levels of testing, infection rates and fatalities.
At the time of publishing, the DRC has reported a record number of cases in the ongoing outbreak, which has so far caused a confirmed 782 cases and at least 181 deaths as of June 13. Suspected infections and deaths are even higher. The vast majority of cases have been in the DRC’s province of Ituri, but infections have also been reported elsewhere in the country, as well as in neighboring Uganda.
This outbreak is different from past Ebola epidemics: the Bundibugyo virus is less understood, having caused just two outbreaks before now. And there are no approved vaccines or treatments for this kind of Ebola (although several vaccine candidates are in development). The outbreak also went undetected for some time, allowing it to grow at remarkable speed.
On supporting science journalism
If you're enjoying this article, consider supporting our award-winning journalism by subscribing. By purchasing a subscription you are helping to ensure the future of impactful stories about the discoveries and ideas shaping our world today.
“I think the reason why alarm bells really rang at the beginning of this [outbreak] was the size that it was at the time of detection,” says Ruth McCabe, a public health researcher who conducted the research while at the School of Public Health at Imperial College London. Compared with previous Ebola outbreaks, she says, “this was detected late, and that is alarming.”
McCabe is a co-author of a new study, published last week in the Lancet Infectious Diseases, that aims to estimate the size of the outbreak based on different assumptions about the levels of testing, growth rates and fatality rates of the virus that is driving it.
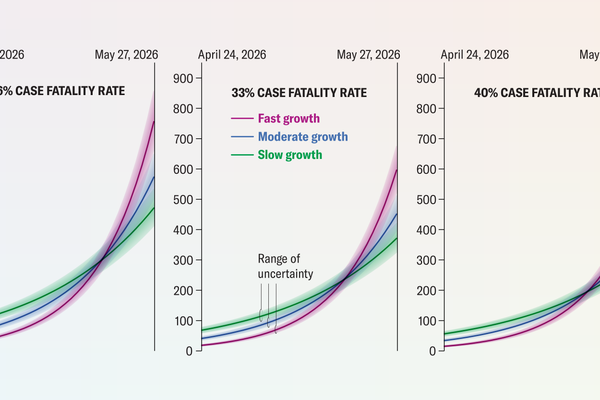
She and her colleagues used two different methods to estimate the scope of the outbreak. The first model was based on reports of suspected and confirmed deaths as of May 27, with the assumption of a time period from symptom onset to death of 11.37 days. Because the actual fatality rate of the Bundibugyo virus isn’t clear, the authors made three calculations based on fatality rates of 26 percent, 33 percent and 40 percent. They compared cases for moderate, fast and slow growth, with doubling times of 10, seven and 14 days, respectively.

The second model was based on geographic spread of the virus as people traveled from the DRC’s provinces of Ituri and Nord Kivu across the border to Uganda. There were three confirmed imported cases of Ebola reported in Uganda as of May 27. Again, the researchers calculated case numbers for moderate, fast and slow growth scenarios based on cases imported from Ituri alone versus Ituri and Nord Kivu.

Both methods produced fairly consistent estimates for the size of the outbreak as of May 27. The first model yielded an estimate of between 306 and 2,521 cases, whereas the geographic spread model estimated between 282 and 1,345 cases. The researchers stress that these estimates have a lot of uncertainty and that many cases could be missed. “The broad convergence of our estimates from two independent methods supports the conclusion of potentially substantial underdetection of cases and the potential for wider transmission,” the authors wrote in the study.
Tracking the number of cases and deaths in Ebola outbreaks is notoriously difficult, complicated by weak public health systems, armed conflict and other factors. That makes comparisons between the current situation and past Ebola outbreaks almost impossible, McCabe says.
To better understand how big the current outbreak could get and how long it might last, researchers need more accurate information about how transmissible the virus is, McCabe says, adding, “That is the next step.”
